Breast enhancement has been one of the most popular plastic surgery procedures since my practice began in 1973. But the goal is to do more than simply enlarge the breast; it is to make the breast beautiful. Most, but not everyone, believe that a breast should look natural. This means that the nipple-areolar complex (NAC) should be centered on the breast mound. If the implant is placed too high, the nipple will point downward; if it is too low, it will point up: if too close to the center, the nipple points outward, and so forth. Ideally, it should look and feel like a breast, and it should move like a breast and not be so firmly fixed to the chest wall. `
There are many choices about implant type and placement, and they all can affect the outcome, such as silicone vs. saline implants, behind or in front of the muscle, the size and shape of the implant, whether or not to perform an uplift, and how to keep the encapsulation rate as close to zero as possible.
Silicone implants are now cohesive, meaning if the shell tears, the silicone gel will not leak out. If saline implants leak, they will go flat. If a patient has very little breast tissue, the saline implants frequently demonstrate wrinkles, which can be seen and felt. Gel implants feel more natural, but saline implants are less expensive.
Implant position should be discussed with your plastic surgeon. Many like the submuscular position for the implant. I prefer to tailor the procedure to the patient and the patient’s activities. If there were a perfect method, there would only be one option. The submuscular position may have a lower encapsulation rate, but the recovery time is a little longer, and the implants cannot be placed as close to the midline in many people. Also they may move outward when the pectoralis muscle is used or flexed.
Encapsulation occurs when the body forms scar tissue around the implant, which begins to squeeze the implant making it look like a ball and feel hard to the touch. In my opinion this is scar tissue formation from bacteria and/or something on the implant such as powder, lint or blood. Preventing an encapsulation has been one of the most challenging obstacles for plastic surgeons. To help prevent this from happening, I personally use powderless gloves and use fresh gloves after dissecting the skin and before I touch the implants. I also use an antibiotic solution in the dissected pocket of the breast tissue. Being very careful with these and other small details has given my patients a very low encapsulation rate. As they say, “the devil is in the details.”
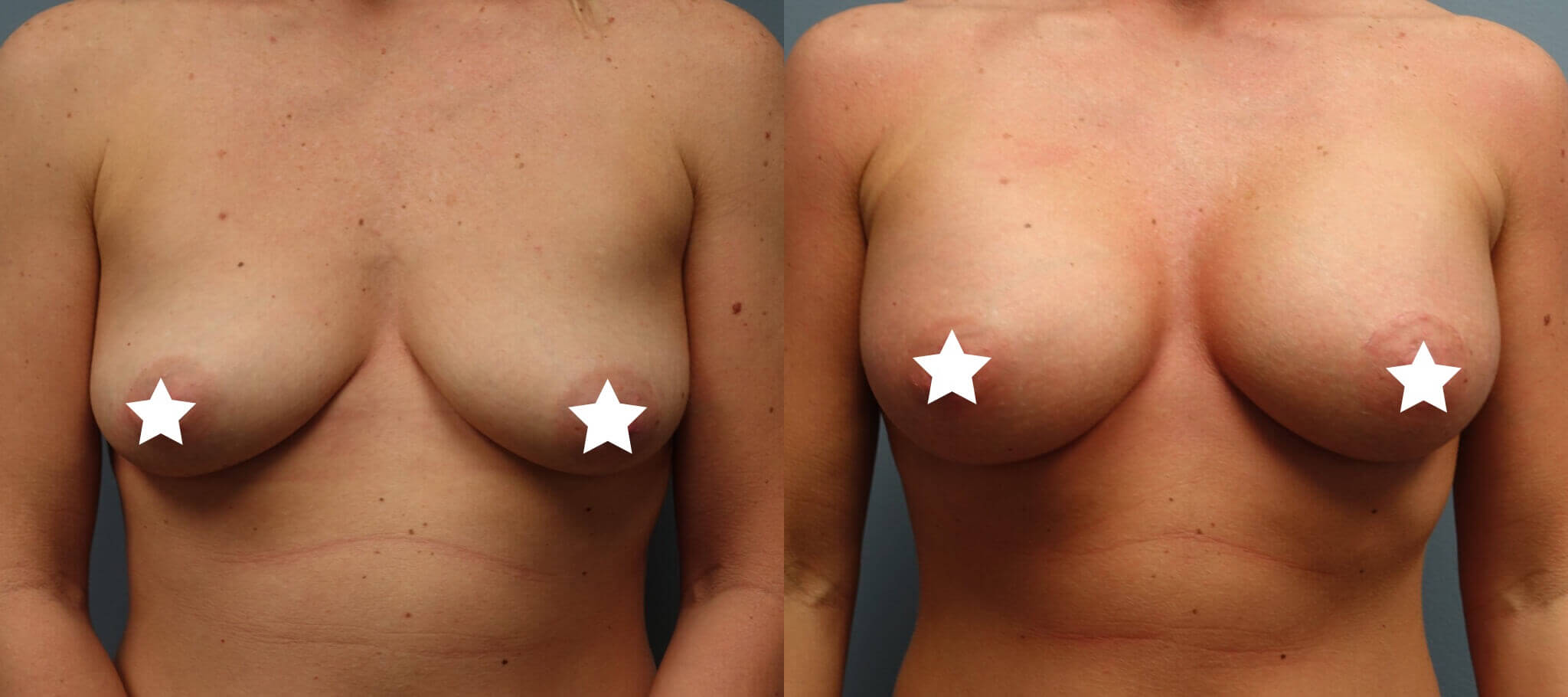
If a patient has excess sagging of the breasts, it may be necessary to perform a breast uplift (mastopexy) with insertion of breast implants. Simply putting in larger implants can lead to an unfavorable result. If the nipple is below the inframammary crease then a mastopexy is recommended. If a patient has enough breast tissue, an auto-augmentation can be done (auto stands for autologous). This means a mastopexy can be done using the patient’s own tissue for fullness instead of an implant.
What about Fat Transfer for breast enhancement? It is probably the future for reconstruction of the breast and even in a cosmetic augmentation when going up one or two cup sizes. Years ago, plastic surgeon’s tried using a patient’s own fat which was liposuctioned from the abdomen, sides or thigh area. The results at that time were largely unsatisfactory, and the procedure was mostly abandoned. Recently, with the emergence of liposuction equipment such as the “Tickle Lipo,” advanced centrifuging techniques, and preservation of the regenerative fat cells (stem cells), fat transfer to the breasts is shown to be extremely effective with long lasting results. Only one to two cups size increase can be done, but the upside is no foreign body in the breast. For those patients with issues of firm implants due to a repeated encapsulation, this is an effective new alternative. Other indications are patients having a mastopexy who want more fullness in the top of the breast or in breast reconstruction patients.