

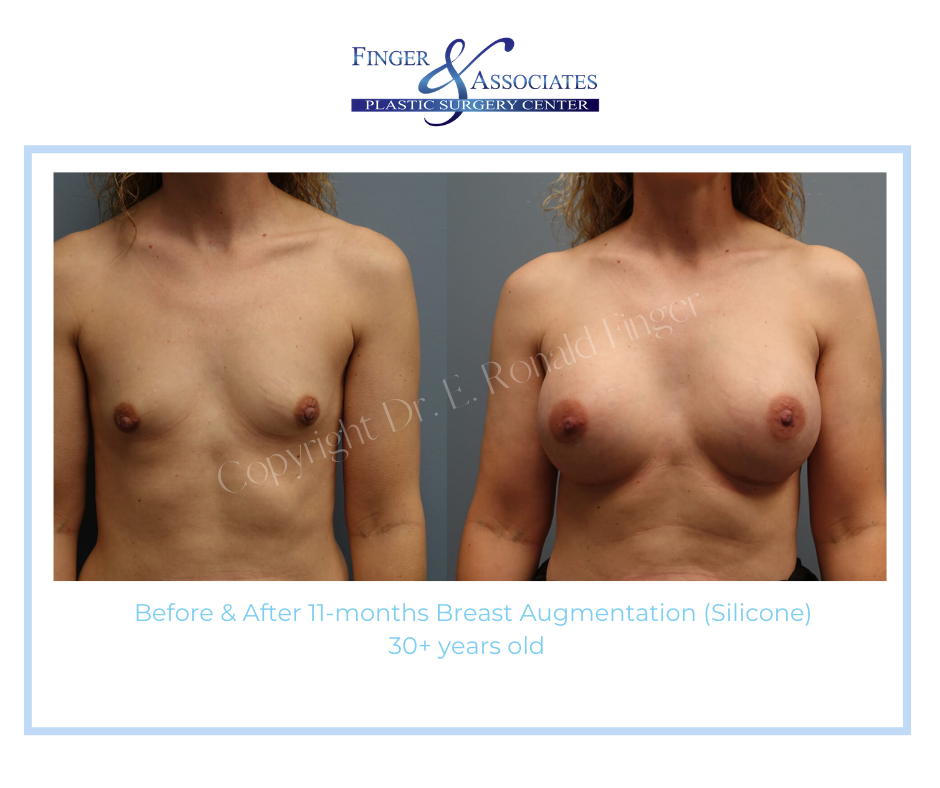
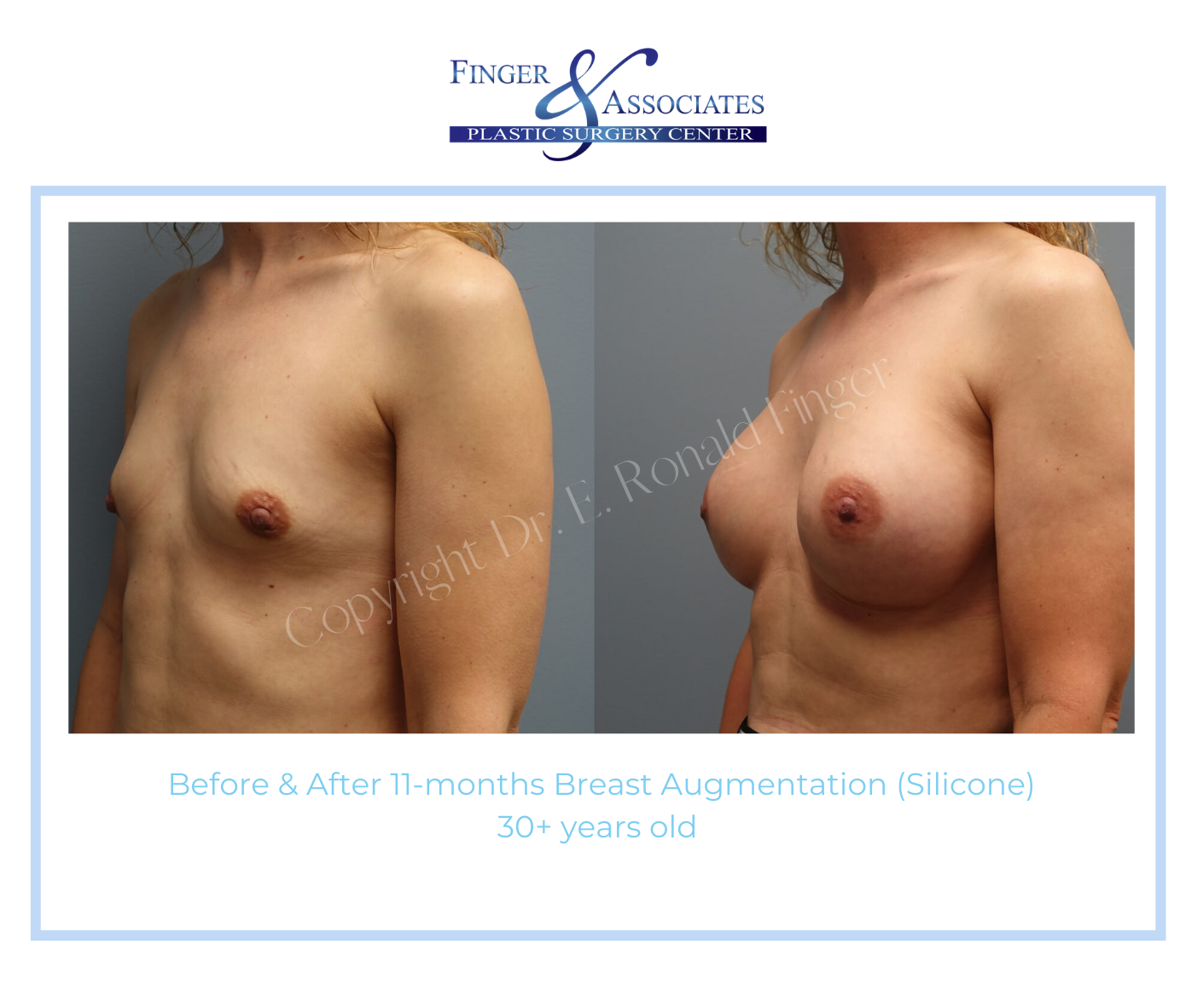
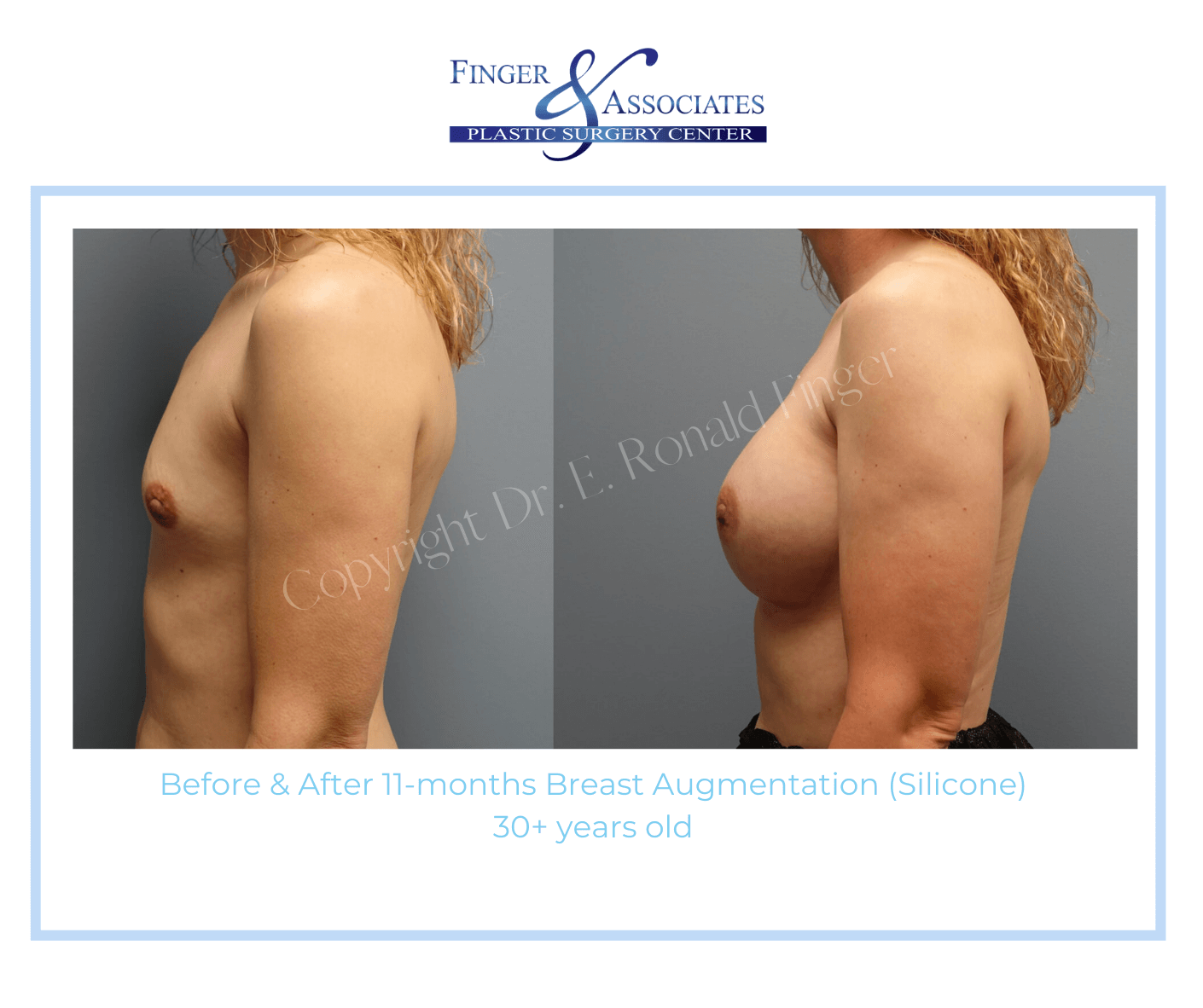
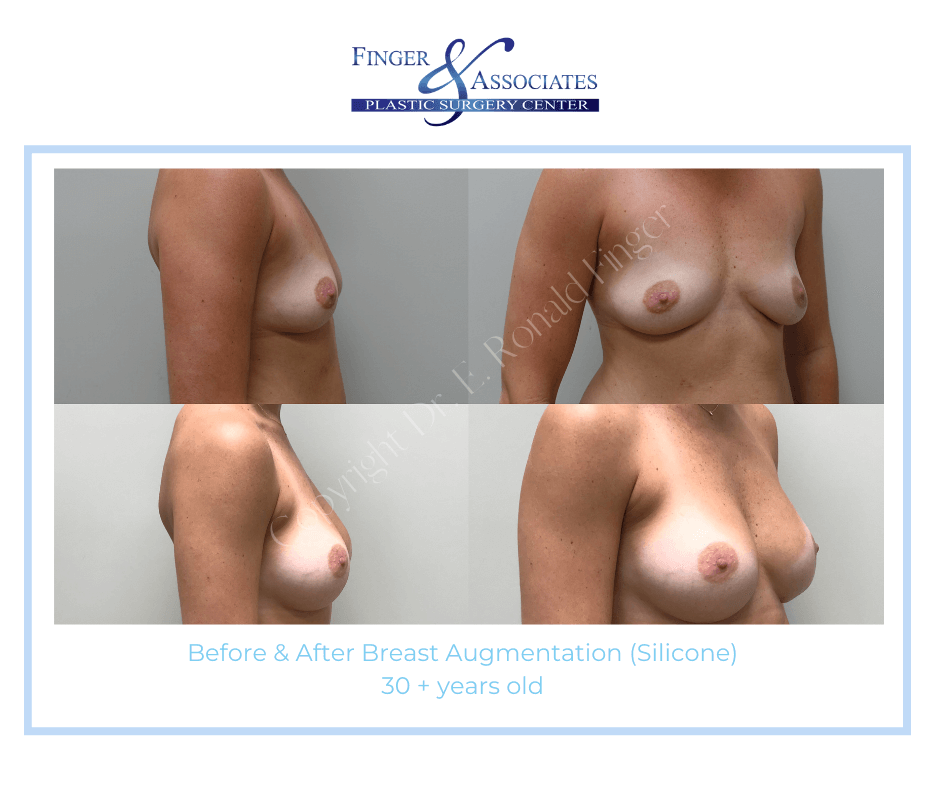
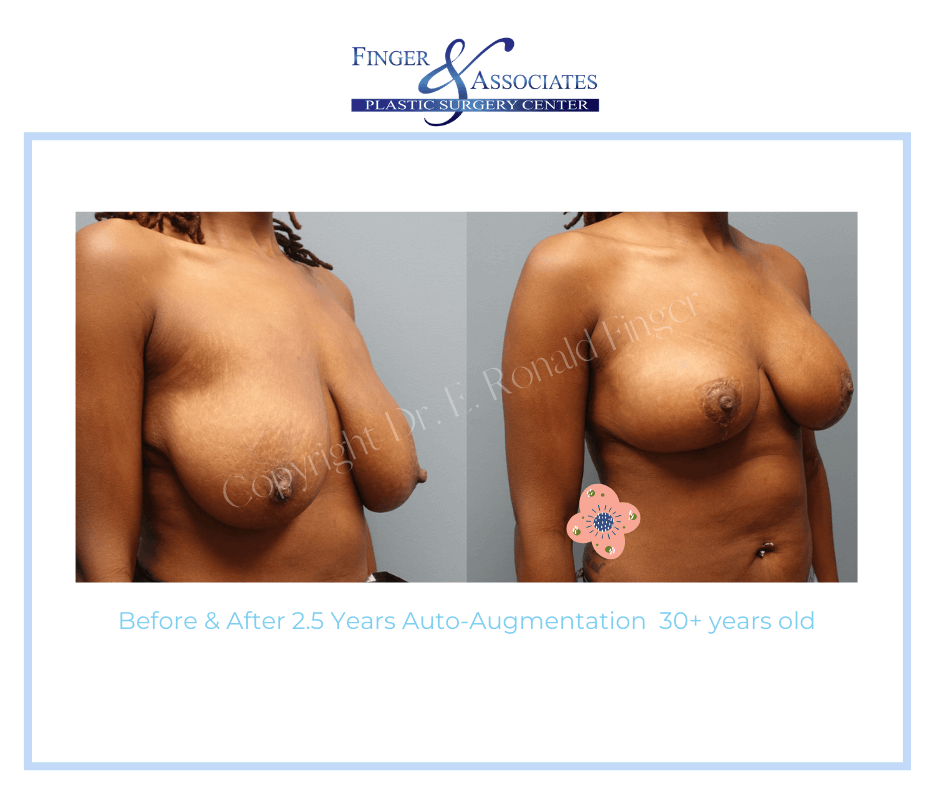
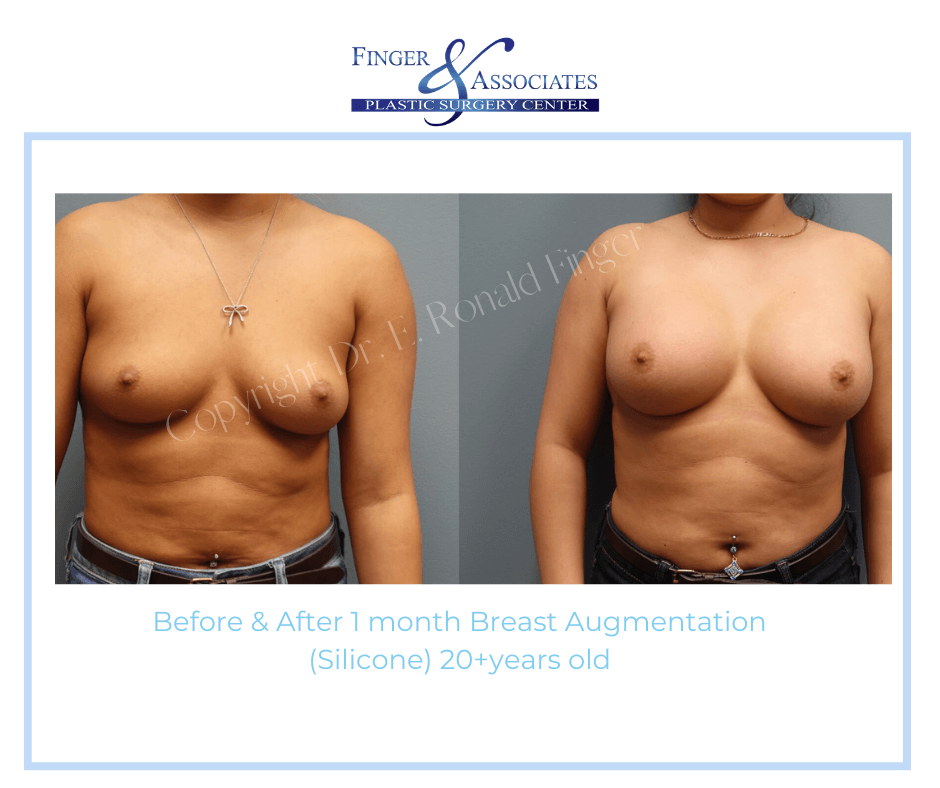
Breast Augmentation Gallery (Mammoplasty)
















Appointment Request
"*" indicates required fields

"*" indicates required fields